MeetYourClinic Editorial Team
Medical Tourism Research · Updated Mar 2026
Quick Summary
A practical guide to hair transplant graft numbers in 2026, including typical ranges by area and Norwood level, what changes your graft count, and the questions to ask before you book.
If you are researching a hair transplant, the first number you usually hear is the graft count. Unfortunately, it is also the easiest number for clinics to oversimplify.
A “graft” is a follicular unit, a naturally occurring bundle of 1 to 4 hairs taken from the donor area and transplanted to thinning or bald areas. Two people with the same Norwood level can need very different graft counts because hair calibre, curl, colour contrast, donor density and goals change how much coverage you get per graft.
Quick Summary
Most first-time hair transplants in men land somewhere between 1,500 and 3,500 grafts, but it is normal to be outside that range.
- Hairline and frontal third usually need higher density than the crown to look natural.
- Crown work is graft-hungry because the swirl pattern spreads grafts over a larger area.
- Ethical planning is not just “how many grafts can we take today”, but how many you should reserve for the future.
- A good plan is based on: measured area (cm²) × target density (grafts/cm²) × a realism check against donor supply.
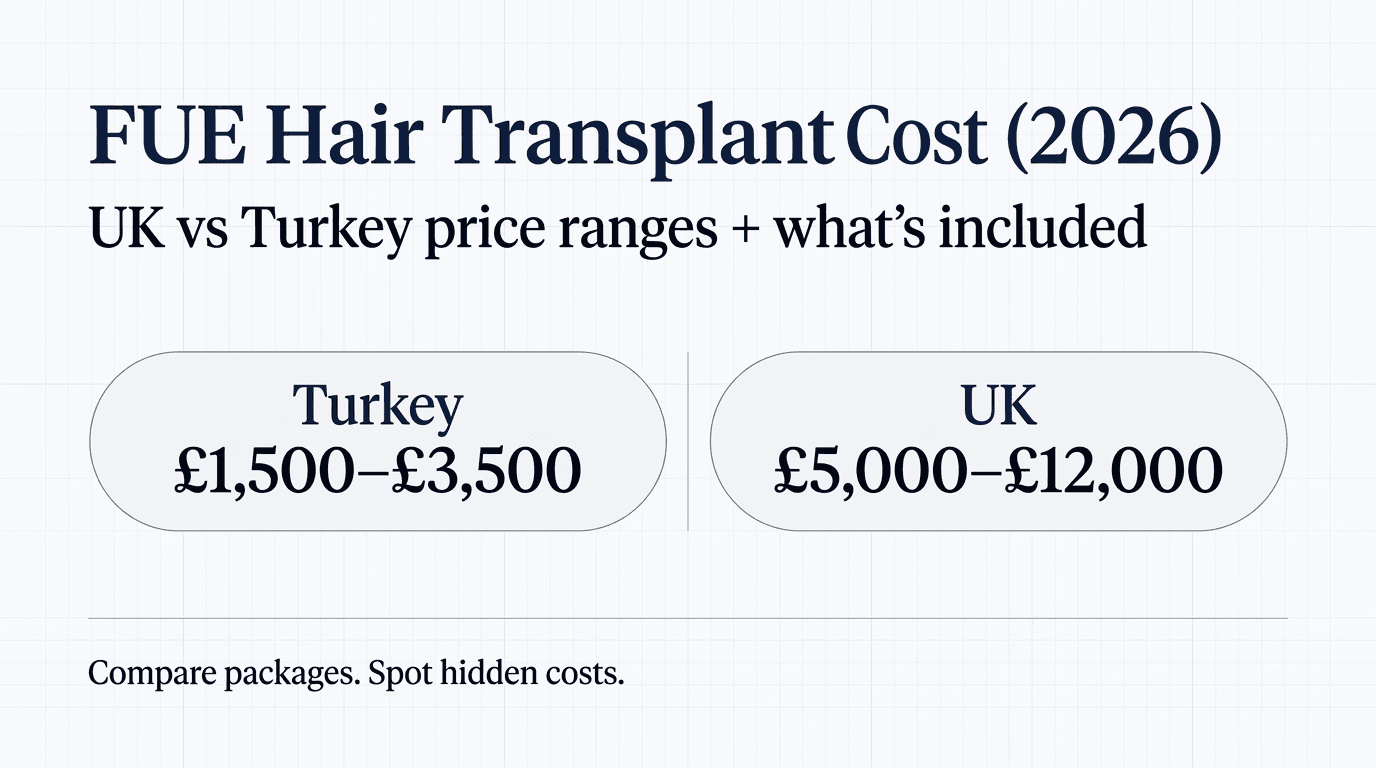
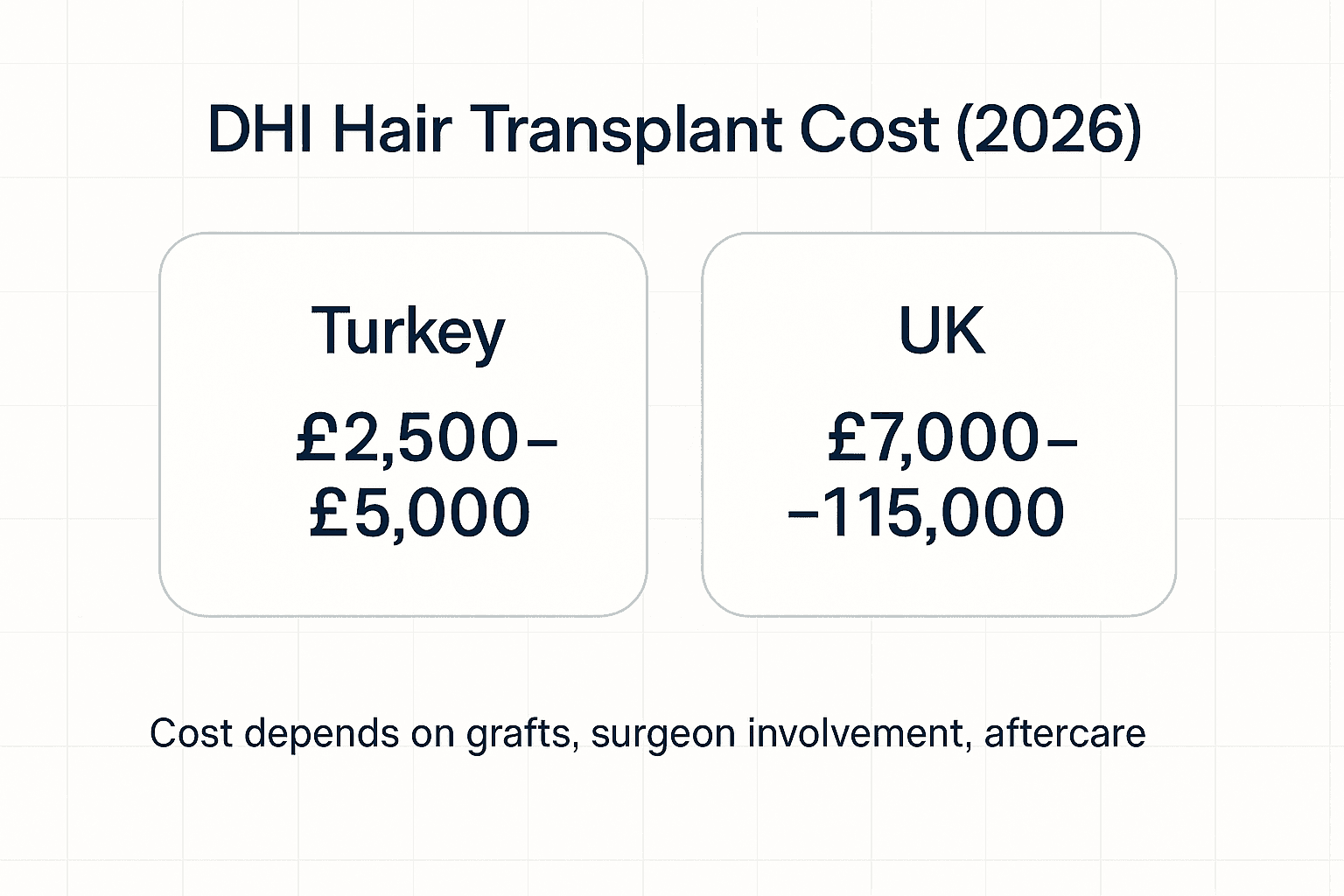
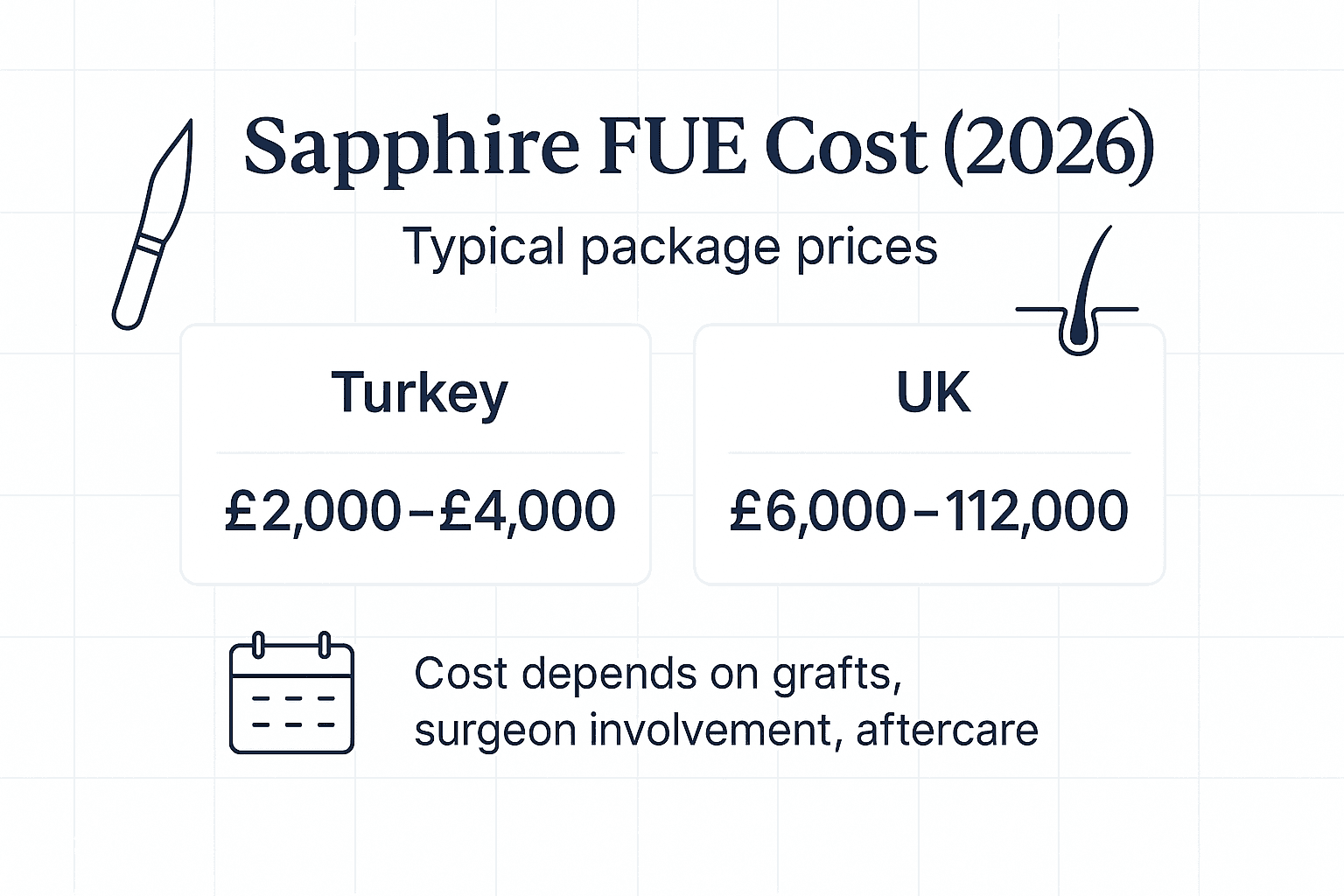
If you also want the financial side, see our guides to cost: /blog/hair-transplant-cost-2026 and /blog/hair-transplant-cost-uk-2026.
What exactly is a graft (and why “hairs” is not the same thing)
Clinics sometimes advertise “4,000 grafts” and sometimes “10,000 hairs”. Those are not interchangeable.
- A graft (follicular unit) may contain 1, 2, 3 or 4 hairs.
- Your average hairs-per-graft depends on genetics and donor characteristics.
- That means 2,500 grafts could be roughly 4,000 to 6,000 hairs for many people, but the exact number varies.
When you compare quotes, compare grafts-to-grafts, and ask the clinic to explain how they estimated the number.
Typical graft ranges by area (simple guide)
These ranges assume adult male-pattern hair loss and an average-size head. They are not a promise. Your surgeon should confirm the actual area and plan using measurements.
Hairline and frontal third
The front frames your face. It is where people notice density changes first, and it is the area where surgeons often aim for a more refined result.
Typical graft ranges (front-focused cases):
| Area | What it includes | Typical graft range |
|---|---|---|
| Hairline “touch-up” | Minor temple/hairline recession with good mid-scalp density | 800 to 1,500 |
| Frontal third | Hairline + immediate forelock and frontal density | 1,500 to 2,500 |
| Frontal + mid-scalp | When thinning extends behind the hairline | 2,500 to 3,500 |
A natural hairline often uses a mixture of single-hair grafts at the very front edge and multi-hair grafts behind to build density.
Crown (vertex)
The crown is more complex than it looks. Hair grows in a swirl, and the balding area can be deceptively large.
| Crown situation | Typical graft range |
|---|---|
| Small crown thinning (not fully bald) | 800 to 1,500 |
| Moderate crown thinning | 1,500 to 2,500 |
| Large crown / bald crown | 2,500 to 3,500+ |
Many reputable surgeons prioritise the front and mid-scalp first, because that is what frames your face, and leave the crown for a second stage if donor supply is limited.
Typical graft ranges by Norwood level (men)
Norwood level is a useful shorthand, but it is not a treatment plan. Two Norwood 4 patients can have different graft needs depending on hair calibre, donor density and whether the crown is involved. The Norwood classification itself comes from classic male-pattern baldness work and is widely used in clinics today. [1]
The table below is a practical starting point for first-pass expectations.
| Norwood level | Common pattern | Typical graft range (first procedure) |
|---|---|---|
| 2 | Mild recession, mostly temples | 800 to 1,500 |
| 3 | Clear temple recession, may include forelock thinning | 1,200 to 2,000 |
| 3V | Front + early crown | 1,800 to 3,000 |
| 4 | Deeper recession, thinning mid-scalp | 2,200 to 3,500 |
| 5 | Front and crown connect (bridge thinning) | 3,500 to 5,000 |
| 6 | Large top area bald | 4,500 to 6,500 |
| 7 | Extensive loss, narrow donor band | 5,500 to 7,500 (often not suitable for full coverage) |
Notes:
- Norwood 6–7 cases are where clinics can overpromise. A safe donor supply may not support full high density everywhere. [2][3]
- Some people are best served by strategic coverage (hairline + forelock) rather than chasing full coverage on the crown.
How clinics calculate graft numbers (the method you want them to explain)
A responsible graft estimate usually has three layers:
1) Measure the area in cm²
The clinic should outline the recipient zones and estimate their surface area (in square centimetres). This can be done with simple measurement tools, digital planning, or photographs with scale references.
2) Choose a target density for each zone
Density is often discussed as grafts per cm². Clinics may use different target densities for the hairline, mid-scalp and crown.
Important: your native hair density (how many follicular units you naturally have per cm² in the donor or non-balding scalp) can be around 60 to 100 follicular units per cm² in many people, which is why transplants typically aim lower than natural density. [2]
In practice, many surgeons aim for cosmetic (not native) density, often with higher density in the front and lower density in the crown, because the crown can consume grafts quickly.
3) Reality-check against donor supply and long-term planning
A good plan matches your goals with what is safe to harvest.
- A donor assessment may include densitometry and an evaluation of the “safe donor area”. [2]
- Overharvesting can permanently thin the donor area and make future procedures difficult. [3]
If you want to understand how technique choices affect planning (especially in the implantation step), see our comparison: /blog/fue-vs-dhi-hair-transplant-2026.
What changes the graft count (why quotes vary so much)
Donor density (how many grafts you can safely take)
Your donor region is not an unlimited bank.
- Higher donor density usually means more available grafts.
- Low density or a narrow safe donor zone reduces capacity.
This is why a clinic should measure your donor characteristics, not guess.
Hair calibre (thickness)
Thicker hair shafts create better coverage per graft. Two people with the same graft count can get visibly different density depending on hair calibre.
Curl and wave
Curly or wavy hair can create more “visual coverage” because it stands off the scalp and overlaps. Straight hair can require a higher graft count to achieve the same cosmetic effect.
Hair-to-skin colour contrast
High contrast (dark hair on light scalp, or light hair on dark scalp) often makes thinning more noticeable. Lower contrast can appear fuller at the same density.
Miniaturisation and diffuse thinning
Diffuse thinning is tricky because you are not transplanting into a completely bald area. You need to avoid shock loss risks, preserve existing hair, and sometimes treat with medication first.
The graft plan may include:
- Lower density “reinforcement” in a thinning zone
- A staged approach (front first, then crown)
Your goals: natural vs dense, and present vs future
Some people want a conservative, age-appropriate hairline and “better than now”. Others want a very dense hairline and are willing to use more grafts.
A good surgeon should talk about:
- Your likely future loss pattern
- Whether you may need a second procedure
- How much donor should be reserved
Ready to Compare Clinics?
Get verified quotes from top-rated hair transplant clinics. Compare prices and reviews in minutes.
Practical graft planning: density, area and a simple formula
A simplified planning approach looks like this:
Estimated grafts = Recipient area (cm²) × Target density (grafts/cm²)
Example target densities (illustrative only):
| Zone | Common planning approach |
|---|---|
| Hairline edge | Lower density with careful singles for a soft, natural transition |
| Frontal third | Moderate-to-higher density for framing |
| Mid-scalp | Moderate density to blend into existing hair |
| Crown | Lower density or staged approach to conserve donor |
The clinic should then stress-test the result against donor limitations and long-term loss.
Worked examples (how the numbers can add up)
These examples show how two people can have different graft needs even if they both “look like a Norwood 4” in photos.
Worked example 1: Frontal third focus (Norwood 3–4 front)
Profile
- 34-year-old man
- Recession at temples and thinning in the forelock
- Crown largely stable
- Medium hair calibre, slight wave
Plan
- Treat frontal third only
- Aim for strong framing, conservative on graft spend
Typical graft range: 1,800 to 2,600
Why: the treated area is limited, and you can concentrate density in the front.
Worked example 2: Front + crown (Norwood 3V–5)
Profile
- 41-year-old man
- Frontal recession plus visible crown thinning
- Dark hair on light scalp (high contrast)
Plan
- Prioritise frontal third and forelock
- Light crown reinforcement rather than full crown build
Typical graft range: 3,000 to 4,500
Why: crown work increases graft demand quickly, even when you keep the crown plan conservative.
Worked example 3: Advanced loss (Norwood 6)
Profile
- 48-year-old man
- Large bald top area
- Donor density average but safe donor zone not particularly wide
Plan
- Build an age-appropriate hairline and dense forelock
- Use mid-scalp coverage to connect the look
- Defer crown density or accept lighter coverage
Typical graft range: 4,500 to 6,000+, often staged
Why: the area is large, and long-term donor safety matters. Overharvesting risk and donor management become central. [2][3]
Questions to ask your clinic (and what a reassuring answer sounds like)
Bring these to your consultation, especially if you are comparing quotes abroad.
How did you calculate my graft number?
- Reassuring: they talk about measured area, zone-by-zone density, and donor assessment.
What is my donor density and hairs-per-graft average?
- Reassuring: they measured it and can explain what it means for planning. [2]
How many grafts do you think I will need in my lifetime?
- Reassuring: they discuss progression, medication, and the importance of reserving donor.
Are you planning singles in the hairline?
- Reassuring: yes, with a natural transition and careful angulation.
Will you work on my crown in the same session, and why?
- Reassuring: they explain the trade-off between crown aesthetics and graft efficiency.
How do you avoid overharvesting?
- Reassuring: they reference safe donor management, extraction distribution, and donor preservation. [3]
Who extracts and who implants the grafts?
- Reassuring: clear roles, surgeon involvement, and realistic daily limits.
What is the plan if I lose more hair later?
- Reassuring: staged strategy and follow-up, not “one and done”.
Donor supply: how many grafts are you likely to have “in the bank”
It is common to focus on the graft count for a single session, but long-term planning matters more. Your donor area contains a finite number of follicular units, and only a portion can be safely moved without visibly thinning the back and sides. Safe donor assessment and careful extraction patterns are central to avoiding a “moth-eaten” look. [2][3]
A clinic cannot give an exact lifetime number from photos alone, but they should be able to explain the logic using donor density measurements (densitometry) and the size of your safe donor zone. [2]
A rough way to think about donor supply is:
- Total donor follicular units (based on measured area and FU density)
- × a conservative extraction percentage spread over the safe zone
- minus what you may want to reserve for future loss
Because follicular unit density varies between individuals, guidelines commonly describe typical scalp FU densities in the region of 60 to 100 FU/cm². [2]
Typical “lifetime” graft availability (very approximate)
These are broad, practical ranges you may hear discussed. They are not a promise and they vary with hairstyle preferences, donor characteristics, and whether you have FUT, FUE or a combination over time.
| Donor situation (simplified) | What it often looks like | Very rough lifetime graft availability |
|---|---|---|
| Low density / narrow safe zone | Thin donor, high contrast, limited flexibility | 2,000 to 4,000 |
| Average donor | Typical density and scalp laxity | 4,000 to 7,000 |
| High density / wide safe zone | Strong donor, good calibre, low contrast | 6,000 to 9,000+ |
If a clinic is suggesting a huge graft count while spending the majority of your donor in one go, it is reasonable to ask how they plan to avoid overharvesting and what they expect your donor to look like at short hair lengths. [3]
Recipient density: why “more grafts” is not always better
Patients often ask for a density that matches their teenage hair. In reality, many transplants aim for cosmetic density, not native density, because the blood supply, recipient site creation, and graft survival can impose practical limits.
Dense packing can be done in selected circumstances, but it is technique- and patient-dependent. One observational study reported high growth rates even at 72 grafts/cm² in a small, tattooed test area in a single patient using the lateral slit technique. [4] That does not mean every scalp, every clinic, or every session can safely aim for that density.
This is why the best plans combine:
- a natural hairline design
- sensible density targets by zone
- realistic expectations based on your hair characteristics and donor supply
Why clinics have “daily graft limits” (and why it matters to you)
Large numbers sound impressive, but there are practical constraints.
In FUE, each follicular unit is extracted individually using small punches (commonly under 1 mm). The technique is effective, but it is labour-intensive and carries a risk of transection (damaging follicles) if speed outruns precision. [5]
A review article on FUE noted that in trained hands it can be possible to achieve more than a thousand grafts in a day, but the emphasis is on methodology and limitations, not just maximising numbers. [5]
When you compare clinics, ask:
- How many grafts do they typically perform per day?
- Who is doing the extraction and implantation?
- What is the plan for breaks, graft hydration, and out-of-body time?
How graft count links to cost (and why “price per graft” can mislead)
Costs are often quoted as:
- A package price (common abroad)
- A price per graft (common in some UK clinics)
The challenge is that graft count is not a pure “more is better” metric. A clinic can inflate graft numbers, or plan density in a way that is not aligned with donor safety.
Use our cost breakdowns to understand typical pricing and what to check in a quote:
- /blog/hair-transplant-cost-2026
- /blog/hair-transplant-cost-uk-2026
FAQs (phrased like real searches)
How many grafts do I need for a hairline?
Many hairline-only cases fall around 800 to 1,500 grafts, but rebuilding a hairline plus forelock often needs 1,500 to 2,500 depending on how far back thinning goes.
How many grafts do I need for the crown?
Small crown thinning might be 800 to 1,500, while a larger or bald crown can be 2,500 to 3,500+. Crown work is often staged to conserve donor.
Is 2,000 grafts enough?
It can be enough for temples and a modest frontal third improvement. It is usually not enough to rebuild the entire front, mid-scalp and crown to high density.
Is 3,000 grafts enough for Norwood 4?
Often yes for a strong front and mid-scalp result, especially if the crown is not the main issue. If the crown is included, you may need more grafts or accept lighter crown coverage.
Is 5,000 grafts a lot?
Yes. It is a large session and not appropriate for everyone. A responsible clinic should explain donor safety, daily limits, and whether staging would be safer.
How many grafts can be taken safely?
It depends on your donor density, safe donor area and extraction pattern. Overharvesting is a known risk and should be actively managed. [2][3]
Why do two clinics give me different graft numbers from the same photos?
Because photos hide key details: actual recipient area, miniaturisation, hair calibre, donor density, and styling. A proper estimate needs measurements and donor assessment.
Do I need more grafts with FUE than FUT?
Sometimes, but not always. Technique choice affects donor management and scarring patterns. Planning is individual. (If you are comparing FUE and DHI implantation methods, see /blog/fue-vs-dhi-hair-transplant-2026.)
Does thick hair reduce the number of grafts I need?
Often yes, because thick shafts give more visual coverage. It does not change the bald area, but it can change the density required for a cosmetic result.
Sources
Norwood, O.T. Male pattern baldness: Classification and incidence. Southern Medical Journal. 1975;68(11):1359–1365. doi:10.1097/00007611-197511000-00009.
International Society of Hair Restoration Surgery (ISHRS). FUE Clinical Practice Guidelines (2019). (Discusses donor assessment and describes typical follicular unit density ranges.) https://ishrs.org/wp-content/uploads/2019/08/July-15-2019-FUE-Guidelines.pdf
ISHRS Hair Transplant Forum International. How to Avoid Overharvesting During Repeat Follicular Unit Excision (FUE). Hair Transplant Forum Int’l. 2018;28(4). https://www.ishrs-htforum.org/content/htfi/28/4/142.full.pdf
Nakatsui, T. et al. Survival of densely packed follicular unit grafts using the lateral slit technique. Dermatologic Surgery. 2008;34(8):1016–1022. doi:10.1111/j.1524-4725.2008.34200.x https://pubmed.ncbi.nlm.nih.gov/18462426/
Dua, A., Dua, K. Follicular Unit Extraction Hair Transplant. Journal of Cutaneous and Aesthetic Surgery. 2010;3(2):76–81. doi:10.4103/0974-2077.69015 https://pmc.ncbi.nlm.nih.gov/articles/PMC2956961/
Ready to Start Your Medical Journey?
Compare clinics, read verified reviews, and get personalised quotes from top medical facilities worldwide. Save up to 70% on your treatment.